
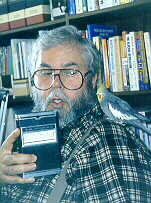
My article
in Diabetes Wellness Letter on "Meter Memories" was only possible because of four great interviews that I was able to obtain. The marketing expert was Charlie Suther, the first patient to use the meter was Dick Bernstein, and the inventor was Tom Clemens. Michael Miller had been credited as the inventor of the first meter, and his interview clarified his role.
Model 5541
Serial 563
Patent Pending
Ames Company, Division Miles Laboratories Inc., Elkhart, Indiana, U.S.A.
I started working on the article as a labor of love even before the magazine gave me the assignment. I realized that the invention of blood glucose meters was extremely important, but little known. In fact, when I started working on it, I didn't even know that the first blood glucose monitor was the Ames Reflectance Meter. Based on what somebody had told me I thought the first meter was the Eyetone and even said that in an article a couple of years earlier.
Very little of the history of blood glucose meters had previously been published. Most important was the introduction to Dr. Bernstein's Diabetes Solution by Richard K. Bernstein, M.D. (Little, Brown, 1997). Dr. Bernstein has also made this available online at http://www.diabetes-normalsugars.com/fiftyyears3.shtml , http://www.diabetes-normalsugars.com/fiftyyears4.shtml , and http://www.diabetes-normalsugars.com/fiftyyears5.shtml .
It was Michael Reynolds, who gave me the lead to Charlie Suther. Michael told me that Charlie was working for Polymer Technology Systems in Indianapolis. In fact, he had retired from that company, but the receptionist told me that he still lived in town.

Click on image to enlarge
The interview with Charlie was extremely productive. Not only does he have a wonderful memory but he also led me to the first patient to use a blood glucose meter. Then he led me—by a circuitous route—to the meter's inventor, Tom Clemens. He didn't know where Tom was any more, but told me that his daughter, who happens to be the First Lady of Nebraska (Stephanie Johans, the wife of the state's governor), was a good friend of Tom's daughter Martina Clemens. Charlie called Stephanie for me and got Martina's phone number, and she gave me Tom's number.
Telephone Interview
With
Charles A. Suther
7857 Trotwood Circle
Indianapolis, IN 46256-4024
(317) 595-0798
September 16, 1999
Starting at the very beginning, Ames developed and introduced in 1965 a product called Dextrostix®. These were paper strips to which you added a drop of blood, timed it for 1 minute and washed it off. They developed a blue color and you read that color by comparing it to a color chart. It gave you an approximation of the blood glucose level. People who did it on a regular basis frequently got to read Dextrostix strips very well. But for most people because of limited usage you could know if it was very high or very low but in between it could be anything. Dextrostix were designed primarily for doctor's offices. Ames had been making urine strips and this was their first excursion into blood glucose strips.
Then in 1970 realizing that the Dextrostix were difficult to use, one of the scientists developed a reflectance meter. That is a meter that could read reflected light.
Who was that? Anton H. Clemens. He developed the first blood glucose meter. And it was simply a light meter that read reflected light. The same Dextrostix were used and the concept was that you play a beam of light on that blue color and the darker the blue the less light would be reflected.
I guess that it didn't give you a number? Oh, yes, it did. That reflected light was sent to a photoelectric cell, which in turn gave a read out, which in this case was a meter with a swinging needle. Since the instrument was more able to read the minor changes in the reflection of the darkness and lightness of the shade of blue it added a certain degree of accuracy. In other words, Dextrostix had been out there for 5 years and now suddenly somebody developed an instrument to read them.
Who developed the Dextrostix? Almost all the stuff developed at Ames Company—and Ames at that time was a division of Miles Laboratories, the Alka-Seltzer people. Ames disappeared, became Miles Diagnostics, and then Bayer bought Miles. So Ames Company, or what's left of it, is now part of Bayer.
So their Glucometers have the oldest history? That's right. They have the history of being the first, the oldest.
What individual was responsible for the Dextrostix? Ernie Adams was the guy at the workbench who invented the Dextrostix. It would be interesting to see whose name the patent is in. [The Dextrostix patent, No. 3,092,465, issued June 4, 1963, is in the name Adams et al.]
Were you there at Ames? Yes, I was there just after Dextrostix were introduced. I started as a sales rep and was later the product manager and still later market manager responsible for diabetes products, including Dextrostix and other diabetes products. That was from 1968-1976 or around there, and I introduced that first reflectance meter.
By the way—they will miss it in a trivia quiz; the name of the first meter was A.R.M., the Ames Reflectance Meter. Because it was a pioneer kind of instrument there were a lot of drawbacks and problems with it. [Anton Clemens writes, "The problems with the ARM was the lead acid battery. We should remember that rechargeable batteries, at that time, had not evolved to the higher tech standards we now take for granted."] Next to the A.R.M. suddenly the Japanese developed an instrument. They called it the Eyetone. The Japanese developed it and brought it to the United States, showed it to Ames Company, and at that point they entered into a marketing agreement. Ames introduced the Eyetone but they didn't develop it.
What Japanese company was that? I believe—I'm sure—it was Kyoto Daiichi.
Was the Eyetone the most important step? It was in terms of popularity. First of all several things happened. The original A.R.M. was very expensive. It was around $495. It was designed for the doctor's office. It was never originally intended for home use. And it was heavy, bulky. The Eyetone was smaller—not by a lot—more lightweight, easier to operate, and most importantly it was less expensive.
What year was the Eyetone introduced? About 1972. It came right on the heals [of the A.R.M.]. It showed up very quickly, whereas it took Ames years to develop the first one. But they didn't violate any patents in doing it (and they sold distribution rights to Ames).
That was a swinging needle too.
That was electrical powered, not battery operated? Right. The A.R.M. was battery operated. It was battery operated, originally with rechargeable batteries, but they had all kinds of problems. The history of the first meter, while the concept was fantastic, the first meter had all kinds of problems.
Is this written anyplace? No I don't think so.
The brought a new level. It was somewhat less expensive. Maybe it was $300. I'm guessing.
[Per Dr. Lebinger at http://www.kwd.org/dteam/1997-03/d_0d_1pb.htm in 1978 the cost of the first commercially available meter, the Eyetone, was US$400.]
At this point, now we are at the very early 70s, people around the world were looking at this thing. They realized that this meter reading of Dextrostix was advantageous.
Did the Eyetone still read Dextrostix? Yes. Now the Dextrostix in and of themselves had some inherent problems. You had to wash it off, put a drop of blood on the strip, wait 50 seconds [Dr. Bernstein says 60 seconds], that was critical, then you washed it off with a stream of water, and then when you used it in the meter you had to blot it. So there were a number of steps you had to do.
These instruments all were being designed for the doctor's office. The ability of a physician to screen patients for blood sugars was something physicians were interested in. it was a way of screening the patient base for high blood sugar and it made a lot of sense. So the developing concept was quite good, but as physicians started to buy and use them there was the strong suggestion that patients might be able to use things and do them on their own would improve their diabetes management.
Was it a prescription item? In the very beginning, not by law but by reason of the Miles legal department. They were quite conservative and when they started talking about selling them to patients the Miles legal department, and we were selling them direct, not through retail outlets, said that you are going to have to get a prescription signed by a doctor saying that they would be responsible for the training.
Were any A.R.M.'s ever sold to individuals? Yes.
When did the first individual buy one and who was that? I was wondering if you were going to ask me that because I happen to know.
I didn't think you would. I do. It is an interesting story in itself and he is one person who I would strongly recommend that you talk to as well. Shortly after the introduction of the A.R.M. I got a phone call while I was working at Ames and it was a guy by the name of Dick Bernstein. He was an engineer and he had seen the meter at a doctor's office or something and he had called me and said he wanted to buy one.
I told him that he would have to get a prescription and all that. He explained that he had had diabetes since he was a teenager and he was averaging one or two hospitalizations [Dr. Bernstein says it wasn't hospitalizations. It was losses of consciousness.] a month, either in diabetic ketoacidosis or hypoglycemia, one or both, [Dr. Bernstein says it wasn't due to diabetic ketoacidosis, it was due to hypoglycemia. One of the main reasons why I started all the blood sugar measurements was all the hypoglycemia. My family was mad at me. I made them miserable, terrified.] and that his diabetes was absolutely impossible for him to manage the way he had been managing it. So we talked a little bit. We had been discussing patient use around Ames in any case, and it turns out that his wife is a psychiatrist M.D., so she wrote the prescription for him. He got his own meter and began testing himself.
We are on the phone six times a month, I would say, he and I, just talking about his experiences. He actually laid the groundwork for much of what happened then in the United States.
But since he had started testing his own blood sugars he was no longer hospitalized, his acne cleared up, he felt better, he experienced a total change in his life. He became a zealot and went all around New York City trying to convince the diabetes guys there they ought to be doing this. He got so involved in it and went at age 47 [Dr. Bernstein says he was 45] to medical school, finished in 3 years and is now a licensed M.D. practicing in Mamaroneck, New York.
He is an old friend of mine and we talk frequently.
When was that that he was the first patient to get an A.R.M.? That was in the early 70s.
That was before the Eyetone came out in 1972? Then he got an Eyetone too. Well, he's had one of every one that's ever been made.
He knew the batteries were a problem with the first A.R.M. What would happen that if the batteries got weak and you didn't realize it, you got bad numbers. So he as an engineer rewired his and made it a plug-in unit. Anyhow, he was one of the first, there was a doctor in Pittsburgh, Pennsylvania, named Ted Danowski, University of Pittsburgh, he was the first to publish a paper in a scientific journal on patient self-testing and what's interesting was that the paper he published had less to do with the testing than they were using an insulin injector and there was some concern about whether they lost some of that insulin to spray when they made the injection. The only way they were going to know was by regularly testing the blood sugar, so they taught a group of 7 or 8 patients how to use the A.R.M.
Was that before Bernstein did? Yeah. No. It was after. What is important about Danowski is that this was the first time in the published medical literature that this idea of testing blood sugar came to the fore.
-
[ Danowski TS and Sunder JH.
Jet injections of insulin during self-monitoring of blood glucose.
Diabetes Care 1:27-33, 1978.]
So Dick Bernstein to our best record was the first individual to do this. Now there were dabblings here and there. For example, Dr. Priscella White at the Joslin Clinic, I think she has passed on now, she was 99 when I met her, in the '60s, right after Dextrostix came out, she was pediatric diabetologist as Joslin and she used to teach the parents of kids with diabetes how to read the Dextrostix visually and we had talked to her about publishing, and she said there was nothing to publish. It would be all anecdotal; there was no formal study, so we had gone to her for some help in establishing the concept of patient testing. Dick Bernstein gave us the first published paper on specifically home testing and then Danowski gave us the first paper published in the scientific press. Bernstein's was sort of a memoir explaining what he did and how he did it. He later got published by Diabetes Care.
Interestingly, we are still at the midpoint of the '70s, Ames was a world-wide company and this idea sort of filtered into Europe, especially England. [Dr. Bernstein says, "It didn't filter. I introduced it to the top endocrinologists in Europe at a meeting in Israel and demonstrated it and got them very excited. I also got the Ames sales manager for Europe and the Near East. That's how penny-ante the whole world was in those days—one sales manager for Europe and the Near East. He was a smart guy, a nice guy, I don't remember his name.] And surprisingly in the early years of blood glucose testing it was more advanced in England that it was here in the United States. Whether that had to do with socialized medicine over there paying for everything or whether it had to do with the way they practiced medicine, I don't know. I have been over there many many times and I have never been able to come back with an answer.
And out of England came a new meter [Dr. Bernstein says this was the Glucochek]. And here again it was an engineer, the father of a diabetic child, saw the Eyetone and he said he could do better than that.
What's his name? I don't know, but somebody in the history of LifeScan would know. I would tell you why, because that was their first meter. Their first meter was developed in England by an electronics company and an electronics engineer and it had been designed to read Dextrostix, of course, and they were looking for a U.S. distribution so some folks out in California, saw this, formed LifeScan company, got the U.S. marketing rights for this meter, but the people at that time did not realize that the money in this business is not in meter. It's in strips. But once they got their hands on them they contacted the Ames Company to private-label the Dextrostix and Ames turned them down.
In the meantime, Boehringer, the German company, Boehringer Mannheim developed a competing blood glucose strip and it was called Chemstrip bG.
Was that a small b, capital G? Yes.
People still write blood glucose that way. That was my name. I gave it that name. In the interim I left Ames and went to Boehringer just as they developed the strip. In my first couple of months on the job they showed it to me and my comment was that it was the strip that Dextrostix wanted to be, much more accurate, much easier. Now you didn't have to wash it off. You put the drop of blood on it, you still had to time it, and then you wiped it off with a ball of cotton or Kleenex. [Dr. Bernstein says, "It was a ball of cotton, not Kleenex, because the Kleenex scratched off the coating and left too much oxygen in. Eventually they modified it so that you could use Kleenex. But with the first Boeringer strips you had to use cotton. You could not use Kleenex, it was too stratchy.] And then you read it visually. And that was an unbelievably easy strip to read visually, because you had two color reference blots, one blue and the other one was beige.
So it showed colors, rather than a number? Right. It was read visually like the Dextrostix.
Why did you make the b small and capitalize the G? That was part of my devious marketing. I wanted to worry the people at Ames Company. I left Ames on good terms, but I wanted to worry them and we started the rumor that the little b, big G indicated the first of a whole series of blood tests, bG for blood glucose, bC for cholesterol, bH for hemoglobin, and there was no such development planned.
People still very often write bG. And then do that not knowing it was just devious marketing.
Now you had two strips on the market. Right around the same time—the mid 70s—the people from LifeScan called Boehringer, they talked to me of course, and they wanted Boehringer to private-label their strip. Their instrument could be made to read either strip. They wanted to read the Boehringer strip and Boehringer turned them down.
So here you had a group of people with the rights to sell an instrument, realizing that the market was going to develop, so you have to give them credit for foresight, they then went to Japan looking for somebody to make strips for them and they found a company, and here you are going to have to get the history from LifeScan, because I don't know it, I just know they went to Japan, found a company. The company not only made them strips but made them the instrument as well. So they never really marketed the instrument from England. Tried, very very spotty, places where they sold it for Dextrostix, but it never really caught on, and they of course to make money had to have their own strip, and that's what they got from the Japanese. And that was the first LifeScan instrument.
That brought it into the patient arena for the first time? LifeScan certainly helped. In the meantime at Ames Company at the time I left, which was in the mid-70s, it was just starting to grab hold. The Boehringer visual strip helped it a great deal, because you could teach patients to read the strip visually without an instrument and there were some people who thought that was advantageous. And so a lot of early glucose testers were testing visually. Dr. Lois Jovanovic, she's out in Santa Barbara at Sansum, but she was at New York Hospital, Cornell University, back in those days, which were the mid-70s, and she had a group of pregnant diabetic women and she managed them through their period of pregnancy and amazing success. She had a concept that women had to use blood glucose meters and strips until they could prove that they were proficient reading them visually. And she called it "freedom from the instrument." Because they felt it was easier. Remember that the instruments were not small. They were fairly sizeable things. Even LifeScan's first one was no miniature. She had a lot of success with the visual meters.
One of the things that really turned this upside down was a very successful symposium paid for by Boehringer Mannheim. Boehringer Mannheim paid for and supported an international symposium on blood glucose management called "Diabetes in the 80s." It was held at Rockefeller University in New York and it was chaired by Charles Peterson, Lois Jovanovic's husband. Chuck Peterson chaired it and there was an international array of speakers talking about where the future of diabetes is going in the next 10 years and as a part of that discussion was the discussion of patient self-monitoring. And that kicked it off, gave it real impetus as far as professional support.
Did you have anything to do with getting that symposium going? It was my idea. I searched out Chuck Peterson and asked him to chair it and he selected Rockefeller University. At that time he had ties to Rockefeller. He and I put together the program and the speaker list. We brought several diabetes specialists in from England and we brought some in from Japan and Canada as well.
And then the president of Boehringer Mannheim U.S. at the time was a fellow by the name of Bill Coll. He's down in Florida somewhere now. He in his position as president had the foresight to know that this market was going to really grow and he shared with me the enthusiasm for the potential of this market. In any case, he not only approved the underwriting of the symposium in New York, he actually arranged, he said that he didn't want to hold this big worldwide symposium and have nobody show up, so he said that we will have every ADA affiliate in the United States. The American Diabetes Association sent two doctors at our expense from every state in the union, one hundred of them, paid all their expenses for this two-day symposium. Surprisingly, especially in New York, the doctors turned out in large numbers.
What year was that? It was 77-78. That's a published hardbound textbook, by the way, edited by Charles Peterson.
Have you written anything about this? No I haven't. But Dick Bernstein called me several weeks ago and called and said that one of his patients said maybe we should write this down and Dick said that I was the one who should write it. But it's never come to be.
The groundswell then was starting. All of these basic instruments were designed for physician office use. And then suddenly in the mid-70s the idea of patient testing starts to grow dramatically. And that has an effect on the later design of instruments. Ames' third generation instrument was the Glucometer and that was really designed; now it was small and compact and more patient oriented. They had the first patient meter.
Boehringer, it took them 6 years to develop a meter to read the Chemstrip bG. That didn't come out until the late 70s. That was the original Accu-Chek.
Glucometer became generic like Kleenex. The Glucometer was also from Kyoto Daiichi.
When was that introduced? I am going to guess. I would say that was about 75.
And then the next one, and by now I had left Ames, and they had several iterations after that, but they went back to their own instrument. In other words, they had two from the Japanese back to back from Kyoto Daiichi, and then they went back to their own design people. I think they called it the Glucometer II.
What about you? Your retired when? Last year, 1998. After about 33 years in the diabetes industry. I joined Ames in 1966 and left in 1973. I left Ames Company in 76 and went to Boehringer. I was at Boehringer Mannheim for 10 years. I left Boehringer Mannheim, and went up to Boston, where I worked with MediSense.
MediSense introduced the first meter that used an entirely different principal. Up until MediSense they all read reflected light. MediSense introduced the first biosensor. That operates on a whole different principal. Very exquisite. And it's been duplicated by every other company.
Is that electro-chemical? Yes, that is the electro-chemical technology.
I was hired by the Boehringer company to put them in the diabetes business. They weren't in that business when I joined them. And then 7 years later it was $100 million. I mention that because I then left Boehringer and went to MediSense. MediSense wasn't in any business before. And in 3 years we reached $100 million. That was a sleighride. It was very exciting. Absolutely superior technology.
What was your career? I was definitely in marketing. A marketing executive.
I didn't catch the first meter with a digital readout? That was the one that LifeScan introduced, I believe the one from England was a digital readout. Before that there was the analog with the sweep of a needle and a scale. Whether it was analog or digital was merely a consumer kind of thing. It had nothing to do with the accuracy. Digital is not better than analog. The A.R.M. in 1970 was the first that could give you a numerical readout. The official name is reflectance photometry.
Those are the two technologies today, reflectance photometry and biosensor or electro-chemical? Yes. And the biosensor approach interesting has been developed by what remains of Ames Company [now Bayer] and LifeScan has a biosensing type.
I understand that Dr. Bernstein uses only the Elite because that is the only one that is accurate. That is such an appropriate description of Dr. Bernstein. He is my dear friend. And we have been friends for years. And I give him this much. Right or wrong when he makes an evaluation of an instrument or system he sticks by it no matter what. They are all about the same.
I left MediSense and started my own consulting business about '92. I did that for a couple of years and that's how I got hooked in to PTS [Polymer Technology Systems]. I worked there fulltime for a couple of years and then I retired.
Telephone Interview
With
Richard K. Bernstein, M.D.
914-698-7500
October 7, 1999
[email protected]
Charlie Suther is a nice guy. Maybe 30 years after he started working with diabetes he developed type 2 diabetes. I've been working on him for years to try my new patent for weight reduction and treating carbohydrate craving.
Many times [self-testing of blood glucose] has been called the most important thing since the discovery of insulin.
I went to medical school because I couldn't get published.
Self-monitoring was especially feared by the ADA. My doctor was the president of the ADA.
Who was he? Max Ellenberg (sp). I can mention his name because he's now deceased. He was very much opposed to self-monitoring. Most of the people connected to the ADA were even viciously opposed. Charlie may not have told you that, but the top people threatened Charlie when he started circulating the self. I published an article, self-published because no one would publish it, on how to normalize blood sugars in type 1 diabetes, and he pedaled the pavement carrying this article. I made a couple of hundred copies. They had to be offset, because we didn't have the kind of copy machines that we have now. We had the thermofax thing. We couldn't get nice copies. He took it around to all the major universities and diabetes investigators and the ADA heard that he was doing that and threatened that if he continued to push self-monitoring, no, if they were to sell a meter to patients that they would formally recommend Lilly's TesTape over the Ames system for testing urine. They had been neutral in the battle between the Ames system and Lilly's TesTape system, but Charlie was told, and you can confirm this with him, that if they were to try to sell the meter to patients, the ADA would recommend the Lilly system over the Ames.
The ADA fought this tooth and nail until they caved in slightly in 1986, I believe it was October. There was a joint meeting of the ADA and AADE, that is representatives of the ADA and AADE and a few other organizations, and by this time the demand from the patients was so great that the ADA caved in and said that they would find self-monitoring as an acceptable mode of treatment for those who take insulin, just those who take insulin, which automatically ruled out 90% of diabetics, and that was in 1986, 17 years after they first knew about it.
When did you get your first meter? I ordered it in 1969, in October or November. And I received it, I believe, in January 1970.
And that was an A.R.M.? Yes, and I have it right up here in my office. I have a museum of all the old meters. That had a built-in battery. And when the reflectance meter came out and I started using it for people‚ two research studies, one at Rockefeller University and one at the downstate division of SUNY, the State University of New York. The reflectance meter was no longer available, and we no longer had a portable meter. So I took battery packs from two 9-volt Radio Shack rechargeable batteries. They needed something like 15 volts, but if you put the two 9-volt meters in series you got 15 volts. And as the patients would be recharging, they had two sets. One would be in the meter and the other would be recharging at home. And I still have one of these little battery packs.
The problem for patients to get one of the early meters is that they had to have a prescription, and you were in the fortunate position that you have an M.D. wife. But which company had the first meter available on a non-prescription basis, and when was that? Okay. I have it right here. It's called the Glucochek. No one in this country wanted me around with this heresy. So I got Zvi Laron in Israel, who still has an annual juvenile diabetes conference. And I sent him this article that I couldn't get published. And he invited me to come and speak at his conference in Israel. And that was around '75 or '76. He had a satellite conference after the main conference for the European Association for the Study of, I think, Pediatric Endocrinology or it may have been Diabetes. I gave a presentation at his main conference and got the Ames people from Europe interested in stocking the meter and making it available to patients. They didn't even have a meter at their booth. They were just selling urine testing. The next conference in Israel a year later they had these meters on display for use by patients. But at the first conference, the small one, the satellite conference, there were some people from England who were very interested in this concept. And they actually got a parent of a diabetic to fund the development by an electronics company of a portable meter, not a big one like the reflectance meter, but a real pocket sized portable meter, and it came out. It was called the Glucochek. That was probably in 1976, maybe 1977. It had one problem. The timer was inaccurate. It had a built-it timer and it was grossly inaccurate. And I still have one here, and here is my calibration curve on the back of it. That was probably '76 or '77. So in England these things were available for patients. The Ames meter was available in England and throughout Europe and the Near East, because of their sales manager, whom I introduced to it. Now, did they do publicity for this? Probably not. But their salesmen were pitching it to the doctors to make available to patients.
When was it first made available in the United States on a non-prescription basis? Probably, I believe they started making smaller meters when I was in medical school. The first one I have here, the Ames Dextrometer came out when I was in medical school. That was probably in 1979. But a prior one, the Ames Glucometer, was available in England at the same time as the Dextrometer was available here. The Glucometer was a superior meter. They did separate consumer research. And you know how these big companies always find out nonsense when they do these consumer research things. They don't ask the right questions. And the Glucometer was developed for use in England because the consumer research was different there than here. And it was a much superior instrument. It was available from Ames in England, deliberately made for consumers around '79, maybe '78, and it didn't became available here until years later, when the found the Dextrometer was a bomb.
Why does the conversation between Dr. Miller in Michigan and Ted Doan considered by several people as the real breakthrough in meters? I would think that it was the breakthrough in bringing LifeScan into the picture. That is probably what it was. LifeScan didn't come out with a meter until I started in practice. That was around '83.
What's special about LifeScan? Was it that they really went after the patients? Their marketing was better? I think it was easier to use and smaller.
And around that time the Accu-Chek series first came out from Boehringer. One of them was superior to the Ames products. The LifeScan products were always mediocre in terms of accuracy. And they still are, but don't quote me.
The Elite is the best one, the most accurate on the market. The Elite has been the best since the first Elite came out. Before that it was the Ames. I was always testing meters, and their meters were not accurate. They are down the road meters. And finally the Elite was fabulous.
One of the main reasons why I started all the blood sugar measurements was all the hypoglycemia. My family was mad at me. I made them miserable, terrified.
My whole reason [for going to medical school] was because I couldn't get published. I tried desperately to get the substance of my first book. I got it boiled down to 10 typewritten pages and no one was interested.
Telephone Interview
With
Anton H. (Tom) Clemens
5854 Schumann Dr
Madison, WI 53711
(608) 273-9772
October 19, 1999
[email protected]
How long have you been in the United States? Since '65.
Did you go to work for Ames right away? Yes. It was part of Miles Labs. I had gotten to know the former Miles management, which at that time was made of primarily by the former owners, the families who started Miles Labs. Miles Labs became a public company, I think in the late '50s. But when I joined them quite a few of its officers were family members. I met them in Switzerland, and they made me an offer that I couldn't refuse to start the instrument program for Miles. And that was within the Ames Division, which was called the professional products division.
What sort of instruments? They were heavily into histology. The [Ames] Reflectance Meter was actually kind of a hobby of mine, which marketing really didn't want to have any part of. We had the Reflectance Meter done, prototypes done, ready for evaluation and I was still ordered at the time by management to quit working on it. [Anton Clemens reviewed the transcript and wrote me on October 20, "We had several prototypes of the Reflectance Meter completed for field trials during the middle of 1968, long before project approval, and the delay to production was out of Instrument R&D's control. My comment about having been ordered to dump an entire project even after we had already completed several prototypes for field evaluation was the arlier mentioned TEC {Tissue Embedding Center}, which only became retroactively approved after a large National Distributor had found out about it and placed a sizable order with the then newly formed Miles Lab Tek Division.]
When was that? I think we had the first prototypes done around '68. There was the new products development committee, which was made up of several different marketing, from finance, manufacturing, and R&D. I had proposed this as a product because I very strongly believed that from an engineering viewpoint it doesn't make any sense whatsoever to take a blood sample to a lab and then have an answer at best in 3-4 hours after and then make any judgment on the diabetes management on the basis of that. I said that if so if it has any merit it should be done on the spot and at the site of the individual and therefore should also be battery operated. One of the higher ups in project management, in fact the highest up, said, "No. If at all it should not be battery operated, it should be line operated." So after we had the first Reflectance Meter on the market; I think it came to the market in '71. Then they took the device to Japan and had a Japanese company make a line operated one, the so-called Eyetone, which was a big flop, and everything went back to battery operated.
The most effective person in marketing to recognize this right away was Charlie Suther. Charlie Suther was the only one initially to side with it.
The chairperson for this new product management committee was a lady, Helen Free. She also was dead set against it. So I placed a bet when we had technical approval. And I said, "Helen, within one year after introduction of this device to the market Dextrostix sales will at least double."
Now, at that time, Dextrostix sales worldwide were just a little more than half a million dollars. Sales not profit. $600,000. She agreed with the wager, which was a bottle of champagne. I won the bet but I never got the bottle.
She and her husband invented the Dextrostix? Actually, that's not true. The one who invested Dextrostix was a man by the name of Ernie Adams [Ernest C. Adams]. Ernie Adams worked for Helen Free.
The Ames Division was started to become a diagnostics product line and was given the name Ames, because Ames was the middle name of the then president of Miles, Walter Ames Compton. He was a member of one of the founding families of Miles Labs. Walter Compton was an M.D., and during his internship became fully aware of the Benedict's solution to test for urine sugar, in which the urine had to be cooked. It must have been a very messy procedure. And since he was fully aware of the effervescent technology of Miles Labs—Alka-Seltzer—and in this effervescent process heat also develops, so he had the idea, but also had the wherewithal within the organization to develop a urine test based on tablets. The Glucotest. So Ames had become conditioned to having urine tests that were based upon the tablet format. And it was Ernie Adams who came up with the idea of putting them on sticks, because it was so much easier to handle. And then when had a few more tests developed in the stick format, Ames then asked him, "Ernie, can't you put it in the tablet format?" But Ernie Adams never got credit for what he did within the Ames organization or in the field in general. Ernie was a very bright individual but was a very shy man and very poor communicator.
Is he still living? I don't know. Ernie would have to be in the late 70s. Now, the Frees were the cheerleaders out at the medical conventions. So they got a lot of credit for stuff that was developed within Ames because those who did the development hardly ever took part in those conventions. So those who talked about it got the credit for it.
Later on within Ames we developed for that time at least a very sophisticated small bench top unit, the urinalysis system. It had a footprint of 4 square feet and was about a foot and one-half high. It processed about a dozen tests and two samples per minute with automatic calibration, the whole bit. It was way ahead of its time.
There was ongoing friction primarily between the Ames Instrument R&D Department, which I was heading, and Ames Marketing, because they would typically want to have a new product after Boehringer had theirs on the market. So reacting but not proacting. Ames did not really capitalize on their pioneer position and allowed Boehringer Mannheim to make big inroads. But then Walter Compton decided that in order to get the best out of both worlds more or less, he decided to have a new business unit, which was structured as a profit and loss center. However, the prime purpose of it was to develop products for life science research with the intent of in so doing that one should then be able to come up with advanced designs and idea that would filter into clinical medicine. Then I was in charge of that unit. In order to facilitate the interaction between the development of instruments and reagents to achieve good 'systems' performance I was, at that time (Ames) Director of Instrument R&D and Associate Director of (Ames) Reagent R&D.
And then out of this, out of Life Science Instruments, that was the name of it, we then put together the first prototype of what eventually became a commercial artificial pancreas, the so-called Biostator® GCIIS (Glucose Controlled Insulin Infusion System). When we had the first production prototype ready, FDA came down with device legislation, and although we had a legitimate order from Washington University in St. Louis to place one, our corporate lawyers didn't feel that this was right. They wanted to live up to the spirit of the law and in the process it cost us 4-5 years. In order to make this program survived we then established an assembly unit in Germany and we assembled about 200 units in Germany for distribution throughout the entire world. That changed more than anything the understanding of glucose control with the visible results that from thereon type 1 diabetics were treating themselves with multiple injections per day instead of one long acting insulin injection. I had 5 or 6 patents on the Biostator system.
How many patents do you have altogether? In the U.S., about 30. I had about a dozen in Europe, before I came here.
Are you a scientist or an engineer? I am an engineer. I have been in the medical field since '51. I came to Ames in '65. I left Ames and set up this different business unit within Miles Labs. My official retirement from Miles Labs was in '87.
Do you consider yourself retired now? I am a buyout retiree, but I will retire when I am 6 foot under.
Are you self-employed? Yes.
Was the meter called the A.R.M. or the Ames Reflectance Meter? Both. In trying to get a trademark established at the time, and it may have been because there wasn't such a big push behind it, there wasn't a big expectation, they did not go for a catchy name that would be a trademark in its own right, since Ames was trademarked they used the Ames name as a vehicle to trademark the A.R.M.
When did you first start working on it? It was at my very first desk [at Ames]. That must have been during '66.
In '68 the first prototype. But it didn't come to market until about '71? Charlie thought it was '70. That's possible. I have the patent here. "Patent issued in '71." I could go back, I may have some numbers in the files. But usually to have a patent issued a year after the introduction is not unusual. So it is likely that it was introduced in 1970.

This was an early prototype of the Ames Reflectance Meter, made when they were considering the use of aluminum extrusion for the case to minimize the tooling cost. This case configuration was also used for the patent application filed on April 22, 1968.
Photo courtesy of Anton H. (Tom) Clemens, the inventor of the Ames Reflectance Meter.
You say it was your hobby. The environment within Miles Labs at the time was a little strange. It was not very conducive to investment-type products, because Miles Laboratories was known for its Alka-Seltzer, its One-a-Day vitamins, and they had some further businesses, but all of these were consumables, which you develop once. And then the "development cost" thereafter is really a marketing expense, advertising and so forth. But the design philosophy for instruments is radically different. Number 1 you have to be prepared for obsolescence, like it or not. If you don't obsolete your product yourself, the competition sure will. So therefore the moment you have a product introduced to the market you have to have already the next generation in the works, and if you don't you'll fall behind. And the other part of it is that in the manufacturing process you need skilled people. And you can only reduce labor content if you go very heavily into robotics to assembly products, but the product volume within the medical diagnostics field at that time, in the '70s, did not justify robotics, so you still were relying on manual assembly, and that was something totally foreign to the mentality of the Miles corporate culture. So it was not an easy task.
If I had waited for approval of every product, we would still be waiting for the first product today.
So you developed the A.R.M. as a hobby without any support? That would be too harsh. Because I had a good financial backing. If I hadn't had the development budget that I had we would not have been able to put together the Reflectance Meter and other products. So there was at the corporate level considerable support, no question about it, but it was an uphill battle for the first several products to get timely approval to go ahead.
Did you ever imagine that blood glucose meters would be so big as they are now? No, not in the dimension that it turned out. However, it was clear to me right from the beginning that this is a niche that will blossom. But I didn't worry about the magnitude at the time.
What was your title there? I was director of instruments in the R&D department and at that time associate director of reagent development.
Someone told me that, "Even Ames was reluctant to promote a self-test for glucose, because they had an attractive reagent franchise in laboratory testing." Is that correct? No. They had an attractive franchise, however their franchise was in the urine testing. Ernie Adams, after he had developed the Dextrostix, Dextrostix sales never took off, because in order to get the value of a blood test it has to be quantitative. The Dextrostix had the potential of being quantitative, but the way it was read did not allow it to be read quantitatively.
This actually was how I got into it. That was one of the reasons I got into it. The Dextrostix had to be read against a color block, a chart that was printed on the label on the bottom. Depending on the light intensity, daylight, incandescent light, fluorescent light, the same color block could look totally different. So therefore it was at the very best semi-quantitative. But if you wanted to control blood sugar ideally close to the normal level, it doesn't do you any good if you have a ±50% readout.
Another problem was in manufacturing. Because in order to produce those Dextrostix reproducibly they had to be tested. And in order to test them they had a group of women who were using batches of Dextrostix and then had light boxes and then did visual readouts against a color block and so one of the first things that became apparent then was that there was no standardization in the color intensity and the characteristics of the light source. And then even thereafter the precision was too poor to make it a good product and then since I was the new kid on the block within the Miles technical community, the manufacturing at that time, and also quality control, was done by the so-called Operating Services Division, which had nothing to do with Ames. The Operating Services Division was in charge of all manufacturing within the Miles organization and one of those section managers of the Dextrostix quality control came and asked me for help how they automate the readout of those Dextrostix. They were using a tristimulous colorometer.
The problem that they had was that the light intensity was so high that the light intensity was driving the reaction and not just the chemistry, because if you have an enzyme test, which the Dextrostix is, if you heat up the process the reaction goes much faster. So they couldn't operate the shutter fast enough to reduce the impact of the light intensity. Then I realized that to have a chance to get a device that would read out the Dextrostix, we would have to reduce the light intensity. And then I found out that the light intensity of a flashlight was plenty to do it.
This led to the idea of making a battery-operated device. I had made the first breadboard, a working model of the Ames Reflectance Meter on my desk. That was, and I remember when, because I know where the first desks were standing, without even a lab, and that was operated by some batteries and a flashlight lamp. Actually it fit into a shoebox. It wasn't a prototype, which requires industrial design. This was a feasibility model. That must have been 1966.
There are two kinds of reflectance.
Charlie says the original A.R.M. was very expensive, around $495. Yes, but that was unfair. That was one of the big issues. Miles had taken people who were producing for other areas and the overhead was just killing everybody. Since that was also used as a negative, "we can't sell it; it is much too expensive," but instead of doing some mea culpa, finding out why it was so expensive, they could have gone outside to get the cost down. We were negotiating with Zenith in Chicago at the time and the industrial designer they had at the time, had connections at Zenith. He was part of my department; I hired him out of Chicago; he had connections to Zenith. They came up with a quote, if I recall correctly, it was $80 for the complete unit, but that was obviously rejected out of hand. It was expensive because it was not manufactured under normal manufacturing conditions.
Charlie says that it was never originally intended for home use. But you had that in mind. We on the development side were proposing it to be marketed for home use. The marketing people took the attitude that they did not want to have the responsibility for a layman to perform a medical test. And for strategic reasons they wanted to engage the medical profession in the mission selling, and that was probably a good move. They did not want to have their customers, that it the physicians take opposition to Ames trying to circumvent them.
Charlie says that it was heavy and bulky. That is not true. Heavy and bulky was the Eyetone. The Eyetone was probably 3 or 4 times heavier than the original. I still have one.
You still have an Eyetone? No I still have a Reflectance Meter.
Do you have a photograph of it? Yes, I'll dig through my files and get some stuff ready for you.
Did you know something personally about diabetes? No, not at the time. The true born engineer has the ability to think in totally abstract terms, very analytical.
The clinical research performed with the Biostator system provided, amongst others, the rationale and the data to perform glucose measurements at fasting, pre-prandially and post prandially (before and one hour after each meal). Therefore, the Biostator system, in a very significant way, contributed to the merits and value of home glucose
monitoring.
But you developed the first blood glucose meter! I can promote both, because I was doing both of them.
Telephone Interview
With
Dr. Michael Miller
Midland, Michigan
September 16, 1999
[email protected]
Let me give you a brief summary of the way it went. I met Mr. Doan at a cocktail party here in Midland. That's where the first conversations came about. He is the former president of the Dow Chemical Company and subsequently chairman of the board of Dow Chemical but he had retired an formed a venture capital company. My wife was involved in some activities at the local center for the arts, the local cultural center, and we were attending a cocktail party for a ballet, where Ronald Reagan's son was part of the ballet at that time. It was about 1980 or 1981.
We started talking about some medical things and they were interested in measuring ionized calcium. They had a company that had an instrument that would measure ionized calcium. So I answered some questions for them about that and gave them my opinions and then I told them that I had been reading about another venture that I think you might be interested in that I think has tremendous potential. And that is self-glucose monitoring for the reasons we all know it is of value. Actually, I can't claim it as my idea in any way because I had read about it in Diabetes Care, I think, which had just started and they had had an issue about the Crock (spelling?) Symposium, where they discussed this issue and they talked about how it was being used in Europe. And where there was a little monitor called the Gluco-Chek (spelling?) and it was apparently built above a habberdashery store somewhere in London and sold on an unofficial basis not in large volumes and there was talk about how the meter might somehow end up in the United States and they were entirely unclear how it might show up in the United States. And there was some talk at that time about the Accu-Chek, not the Accu-Chek. Chemstrip bG. There might have been some talk about that already.
Anyway I told them that I thought this was an idea that might have tremendous value because of the problems of controlling diabetes, because of the problems of measuring glucose in the urine and I caught his ear. He then had another gentleman, a businessman. He and I and some of the people in this venture capital company we got together and we talked about this idea. The other gentleman was Ian Bund, he is an Australian, he still runs a venture capital company in Ann Arbor, Michigan, and you might want to talk to him about this whole thing as well.
The three of us, Mr. Bund, Mr. Doan and I got together. They already had the venture capital company and they worked with another gentleman, out in California, actually he is in one of the suburbs around Mountain View, where LifesScan, was actually set up, Mr. James Weersing, he is a very well know venture capitalist out there, not for computers but for other things. So first we had meetings here, then we got together in Chicago, they bought in Weersing and one or two other venture capitalists and we talked it over. And eventually they hired a young M.B.A. out of the University of Michigan, and he developed a business plan and that eventuated with the incorporation of a company here in Midland, Michigan. It was originally called Diabatech [he's not sure]. We began first with plans to import this meter from England, called the GlucoChek [spelling?] and then began plans to develop our own meter and our own strips.
But it soon became obvious to people who were really well, who had good knowledge of the Silicon Valley and the development of electrical instruments, primarly Mr. Weersing, who ended up being one of the major business movers of the venture. He was eventually chairman of the board of LifeScan during its early phases. They all felt that the company needed to move to California, so it moved to Mountain View, California, where during they early years, until 1986 and somewhat thereafter, after the acquisition by Johnson & Johnson, LifeScan was in Mountain View.
Then it all evolved from their. People were hired. The company expanded. I was on the board of directors as well Mr. Bund. Mr. Doan made some ocassional appearances at the board of directors meetings. Mr. Weersing was the chairman of the board and he became the prime mover. He made trips to England, to Japan, he integrated with the first development of one of the strips we had, with the early meters from the Japanese, we imported the strips from Japan, but eventually they were developed and manufactured at the Mountain View site, we integrated with some of the Silicon Valley companies, like Solectron and other companies regarding the things we needed to develop the blood glucose meter.
We gave the GlucoCheck that name. It was called something else in England.
The very first meter that we developed was a black one. It was called the GlucoScan [he can't remember spelling or when].
You had the original idea for LifeScan? I had the original idea. I participated as a consultant and as a member of the board throughout the development of the company until its sale to Johnson & Johnson in 1986.
So you had a major ownership share in the company? I had a minor ownership.
I would have thought that you made more money from that than your whole medical practice. It did amount to that, but it was still a minor share of the company. At the sale to Johnson & Johnson I owned a little less than 2% of the company.
How much money was that? I don't know if I want that published. It sold for $100 million to Johnson & Johnson.
I am now 56 going on 57 so I was in my late 30s and early 40s when all this was happening.
You had no idea of retiring with that money? It hasn't proved to be enough to do that. So I have had to work and generate other retirement funds and I still want to be an active person, and I am still working harder than you would imagine.I have an active practice called Diabetes and Endocrinology with another associate here in mid-Michigan.I am in group practice here at the hospital, the Mid-Michigan Medical Center. I was in private practice until 3 years ago.
![[Go Back]](back-new.gif) Go back to Home Page
Go back to Home Page
Go back to Diabetes Directory

